Which Theory Supports the Idea That Health Behavior (Good or Bad) Can Be Learned by Watching Others?
Behavioral Change Models
Introduction
Public health is a multi-disciplinary field that aims to 1) prevent disease and death, two) promote a better quality of life, and 3) create environmental weather condition in which people can be healthy past intervening at the institutional, community, and societal level.
Whether public health practitioners can achieve this mission depends upon their ability to accurately identify and define public wellness problems, assess the fundamental causes of these issues, decide populations nigh at-risk, develop and implement theory- and show-based interventions, and evaluate and refine those interventions to ensure that they are achieving their desired outcomes without unwanted negative consequences.
To exist effective in these endeavors, public health practitioners must know how to apply the basic principles, theories, research findings, and methods of the social and behavioral sciences to inform their efforts. A thorough understanding of theories used in public health, which are mainly derived from the social and behavioral sciences, allow practitioners to:
- Assess the primal causes of a public health trouble, and
- Develop interventions to address those problems.
Note: This module has been translated into Estonian past Marie Stefanova. The translation can be accessed at
https://www.bildeleekspert.dk/web log/2018/08/06/sotsiaalsete-normide-teooria/
Learning Objectives
Later successfully reviewing these modules, students volition be able to:
- List and depict the key constructs of the Health Belief Model and the theory of planned beliefs and explain how they might be applied to develop effective public health interventions
- Listing and describe the elements of "perceived behavioral control"
- Describe the underlying theory and basic elements of Social Norms Theory and marketing campaigns
- List and describe the primal constructs of Social Cognitive Theory and explain how they might be practical to develop effective public wellness interventions
- Summarize the criticisms that have been made regarding the major traditional models of health behavior alter and why these models do not seem acceptable to account for observed health behaviors
- Outline the major steps in the Transtheoretical Model
- Listing the characteristics of each pace of the Transtheoretical Model
- Describe Improvidence of Innovation Theory and how it can be practical in health promotion
- Outline the basic structures of the Theory of Gender and Power and its application to Public Health
- Explicate the constructs of the Sexual Health Model and its application to public health
The Health Belief Model
The Health Belief Model (HBM) was developed in the early 1950s by social scientists at the U.South. Public Health Service in order to understand the failure of people to adopt disease prevention strategies or screening tests for the early detection of disease. Later uses of HBM were for patients' responses to symptoms and compliance with medical treatments. The HBM suggests that a person's conventionalities in a personal threat of an affliction or disease together with a person's conventionalities in the effectiveness of the recommended health behavior or activeness will predict the likelihood the person will adopt the beliefs.
The HBM derives from psychological and behavioral theory with the foundation that the two components of health-related beliefs are 1) the desire to avoid illness, or conversely get well if already sick; and, ii) the belief that a specific health activeness volition forbid, or cure, disease. Ultimately, an private'south course of action often depends on the person's perceptions of the benefits and barriers related to health behavior. There are half-dozen constructs of the HBM. The first four constructs were adult as the original tenets of the HBM. The final two were added as research about the HBM evolved.
- Perceived susceptibility - This refers to a person's subjective perception of the risk of acquiring an illness or disease. There is wide variation in a person's feelings of personal vulnerability to an illness or affliction.
- Perceived severity - This refers to a person'southward feelings on the seriousness of contracting an disease or illness (or leaving the illness or illness untreated). There is wide variation in a person's feelings of severity, and often a person considers the medical consequences (e.g., death, disability) and social consequences (e.g., family life, social relationships) when evaluating the severity.
- Perceived benefits - This refers to a person's perception of the effectiveness of various actions bachelor to reduce the threat of affliction or disease (or to cure illness or affliction). The class of action a person takes in preventing (or curing) illness or disease relies on consideration and evaluation of both perceived susceptibility and perceived benefit, such that the person would accept the recommended health activity if it was perceived equally beneficial.
- Perceived barriers - This refers to a person's feelings on the obstacles to performing a recommended wellness activity. At that place is wide variation in a person's feelings of barriers, or impediments, which pb to a cost/benefit analysis. The person weighs the effectiveness of the actions against the perceptions that it may exist expensive, dangerous (e.grand., side effects), unpleasant (e.g., painful), time-consuming, or inconvenient.
- Cue to action - This is the stimulus needed to trigger the determination-making process to have a recommended health action. These cues can be internal (eastward.1000., breast pains, wheezing, etc.) or external (e.one thousand., advice from others, affliction of family fellow member, newspaper article, etc.).
- Self-efficacy - This refers to the level of a person'southward confidence in his or her power to successfully perform a behavior. This construct was added to the model nearly recently in mid-1980. Cocky-efficacy is a construct in many behavioral theories as it directly relates to whether a person performs the desired behavior.
Limitations of Health Belief Model
There are several limitations of the HBM which limit its utility in public health. Limitations of the model include the post-obit:
- It does not account for a person'south attitudes, behavior, or other private determinants that dictate a person's credence of a wellness behavior.
- Information technology does not accept into account behaviors that are habitual and thus may inform the decision-making process to accept a recommended action (e.g., smoking).
- It does not accept into account behaviors that are performed for not-health related reasons such as social acceptability.
- It does non account for ecology or economical factors that may prohibit or promote the recommended activeness.
- It assumes that everyone has admission to equal amounts of data on the illness or illness.
- It assumes that cues to action are widely prevalent in encouraging people to act and that "health" actions are the main goal in the decision-making process.
The HBM is more than descriptive than explanatory, and does not suggest a strategy for changing health-related actions. In preventive health behaviors, early studies showed that perceived susceptibility, benefits, and barriers were consistently associated with the desired health behavior; perceived severity was less often associated with the desired health behavior. The private constructs are useful, depending on the health outcome of involvement, merely for the most effective use of the model information technology should be integrated with other models that account for the environmental context and suggest strategies for modify.
The Theory of Planned Behavior
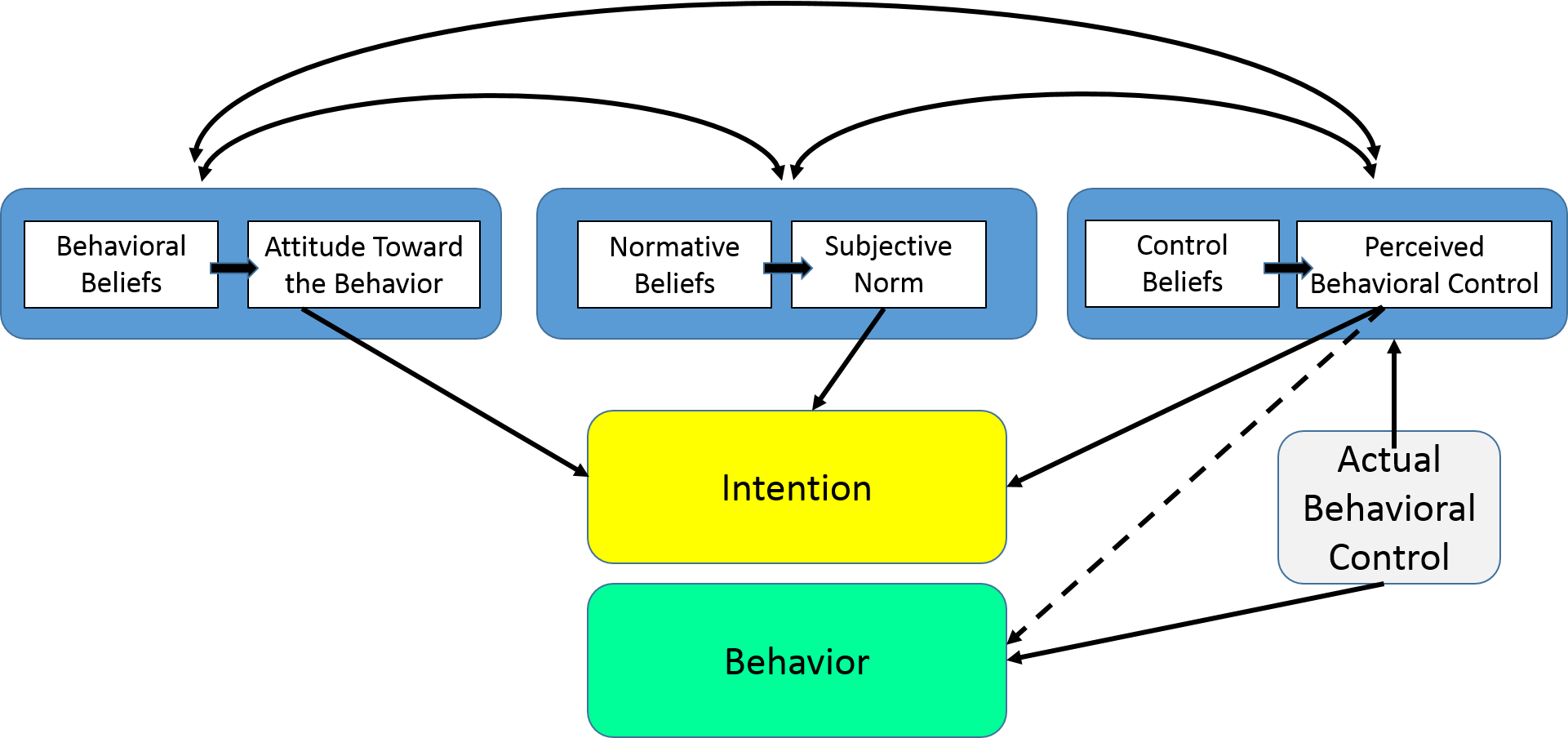
The Theory of Planned Behavior (TPB) started as the Theory of Reasoned Action in 1980 to predict an individual's intention to engage in a beliefs at a specific time and place. The theory was intended to explain all behaviors over which people take the ability to exert self-control. The key component to this model is behavioral intent; behavioral intentions are influenced by the attitude about the likelihood that the behavior will accept the expected outcome and the subjective evaluation of the risks and benefits of that outcome.
The TPB has been used successfully to predict and explain a wide range of health behaviors and intentions including smoking, drinking, health services utilization, breastfeeding, and substance utilize, among others. The TPB states that behavioral achievement depends on both motivation (intention) and ability (behavioral command). It distinguishes between 3 types of beliefs - behavioral, normative, and control. The TPB is comprised of six constructs that collectively correspond a person's actual control over the behavior.
- Attitudes - This refers to the degree to which a person has a favorable or unfavorable evaluation of the behavior of interest. It entails a consideration of the outcomes of performing the beliefs.
- Behavioral intention - This refers to the motivational factors that influence a given beliefs where the stronger the intention to perform the behavior, the more likely the behavior will exist performed.
- Subjective norms - This refers to the conventionalities about whether most people corroborate or disapprove of the behavior. It relates to a person's beliefs virtually whether peers and people of importance to the person call up he or she should engage in the beliefs.
- Social norms - This refers to the customary codes of behavior in a group or people or larger cultural context. Social norms are considered normative, or standard, in a group of people.
- Perceived power - This refers to the perceived presence of factors that may facilitate or impede performance of a beliefs. Perceived power contributes to a person's perceived behavioral control over each of those factors.
- Perceived behavioral control - This refers to a person's perception of the ease or difficulty of performing the behavior of involvement. Perceived behavioral control varies across situations and actions, which results in a person having varying perceptions of behavioral command depending on the situation. This construct of the theory was added later, and created the shift from the Theory of Reasoned Activity to the Theory of Planned Behavior.
Limitations of the Theory of Planned Behavior
There are several limitations of the TPB, which include the post-obit:
- It assumes the person has acquired the opportunities and resources to be successful in performing the desired behavior, regardless of the intention.
- It does not account for other variables that gene into behavioral intention and motivation, such as fear, threat, mood, or past experience.
- While it does consider normative influences, it yet does not take into account environmental or economical factors that may influence a person's intention to perform a behavior.
- It assumes that behavior is the result of a linear controlling procedure, and does not consider that information technology can alter over fourth dimension.
- While the added construct of perceived behavioral control was an important improver to the theory, information technology doesn't say annihilation about bodily control over beliefs.
- The fourth dimension frame between "intent" and "behavioral action" is not addressed by the theory.
The TPB has shown more than utility in public wellness than the Wellness Belief Model, but it is however limiting in its inability to consider environmental and economic influences. Over the past several years, researchers have used some constructs of the TPB and added other components from behavioral theory to make it a more integrated model. This has been in response to some of the limitations of the TPB in addressing public health issues.
Improvidence of Innovation Theory
Improvidence of Innovation (DOI) Theory, adult by East.M. Rogers in 1962, is i of the oldest social science theories. Information technology originated in communication to explain how, over fourth dimension, an idea or product gains momentum and diffuses (or spreads) through a specific population or social organisation. The stop result of this diffusion is that people, as part of a social organisation, adopt a new idea, behavior, or product. Adoption means that a person does something differently than what they had previously (i.e., purchase or utilise a new production, acquire and perform a new beliefs, etc.). The key to adoption is that the person must perceive the idea, behavior, or product as new or innovative. Information technology is through this that diffusion is possible.
Adoption of a new idea, behavior, or product (i.e., "innovation") does not happen simultaneously in a social arrangement; rather it is a process whereby some people are more than apt to adopt the innovation than others. Researchers have plant that people who adopt an innovation early accept different characteristics than people who adopt an innovation later. When promoting an innovation to a target population, it is important to understand the characteristics of the target population that will help or hinder adoption of the innovation. There are v established adopter categories, and while the majority of the general population tends to autumn in the eye categories, it is still necessary to understand the characteristics of the target population. When promoting an innovation, there are unlike strategies used to appeal to the dissimilar adopter categories.
- Innovators - These are people who want to be the first to effort the innovation. They are venturesome and interested in new ideas. These people are very willing to have risks, and are often the beginning to develop new ideas. Very trivial, if anything, needs to be done to appeal to this population.
- Early Adopters - These are people who represent opinion leaders. They enjoy leadership roles, and embrace change opportunities. They are already aware of the need to alter and and then are very comfy adopting new ideas. Strategies to entreatment to this population include how-to manuals and data sheets on implementation. They exercise not demand information to convince them to change.
- Early Majority - These people are rarely leaders, but they do prefer new ideas before the average person. That said, they typically need to see evidence that the innovation works earlier they are willing to adopt it. Strategies to entreatment to this population include success stories and prove of the innovation'south effectiveness.
- Belatedly Majority - These people are skeptical of change, and volition only adopt an innovation afterwards it has been tried by the majority. Strategies to entreatment to this population include data on how many other people take tried the innovation and accept adopted it successfully.
- Laggards - These people are bound by tradition and very bourgeois. They are very skeptical of modify and are the hardest grouping to bring on board. Strategies to entreatment to this population include statistics, fear appeals, and pressure from people in the other adopter groups.

Source: http://weblog.leanmonitor.com/early-adopters-allies-launching-product/
The stages by which a person adopts an innovation, and whereby diffusion is accomplished, include awareness of the demand for an innovation, decision to adopt (or decline) the innovation, initial apply of the innovation to test it, and continued apply of the innovation. There are five main factors that influence adoption of an innovation, and each of these factors is at play to a different extent in the five adopter categories.
- Relative Advantage - The degree to which an innovation is seen as better than the idea, program, or production it replaces.
- Compatibility - How consistent the innovation is with the values, experiences, and needs of the potential adopters.
- Complexity - How hard the innovation is to understand and/or use.
- Triability - The extent to which the innovation can be tested or experimented with before a commitment to adopt is made.
- Observability - The extent to which the innovation provides tangible results.
Limitations of Diffusion of Innovation Theory
In that location are several limitations of Diffusion of Innovation Theory, which include the following:
- Much of the evidence for this theory, including the adopter categories, did not originate in public health and it was non developed to explicitly apply to adoption of new behaviors or health innovations.
- It does not foster a participatory approach to adoption of a public health programme.
- It works amend with adoption of behaviors rather than cessation or prevention of behaviors.
- It doesn't take into business relationship an individual'southward resources or social support to adopt the new behavior (or innovation).
This theory has been used successfully in many fields including communication, agriculture, public wellness, criminal justice, social work, and marketing. In public health, Diffusion of Innovation Theory is used to accelerate the adoption of important public health programs that typically aim to modify the behavior of a social system. For example, an intervention to address a public health problem is adult, and the intervention is promoted to people in a social system with the goal of adoption (based on Diffusion of Innovation Theory). The most successful adoption of a public health program results from agreement the target population and the factors influencing their charge per unit of adoption.
For more on diffusion of innovation theory run into "On the Improvidence of Innovations: How New Ideas Spread" by Leif Singer.
The Social Cerebral Theory
Social Cerebral Theory (SCT) started as the Social Learning Theory (SLT) in the 1960s by Albert Bandura. It developed into the SCT in 1986 and posits that learning occurs in a social context with a dynamic and reciprocal interaction of the person, environment, and behavior. The unique feature of SCT is the emphasis on social influence and its emphasis on external and internal social reinforcement. SCT considers the unique way in which individuals acquire and maintain behavior, while also because the social environment in which individuals perform the behavior. The theory takes into business relationship a person's by experiences, which gene into whether behavioral action will occur. These past experiences influences reinforcements, expectations, and expectancies, all of which shape whether a person will appoint in a specific behavior and the reasons why a person engages in that behavior.
Many theories of behavior used in wellness promotion do not consider maintenance of behavior, but rather focus on initiating beliefs. This is unfortunate as maintenance of behavior, and non just initiation of behavior, is the true goal in public health. The goal of SCT is to explain how people regulate their behavior through control and reinforcement to achieve goal-directed behavior that can be maintained over time. The kickoff five constructs were developed as part of the SLT; the construct of self-efficacy was added when the theory evolved into SCT.
- Reciprocal Determinism - This is the central concept of SCT. This refers to the dynamic and reciprocal interaction of person (private with a set of learned experiences), environment (external social context), and behavior (responses to stimuli to accomplish goals).
- Behavioral Capability - This refers to a person's actual power to perform a behavior through essential noesis and skills. In order to successfully perform a behavior, a person must know what to do and how to do information technology. People learn from the consequences of their behavior, which also affects the surround in which they live.
- Observational Learning - This asserts that people can witness and observe a behavior conducted by others, and so reproduce those actions. This is often exhibited through "modeling" of behaviors. If individuals see successful demonstration of a behavior, they can also complete the behavior successfully.
- Reinforcements - This refers to the internal or external responses to a person's behavior that affect the likelihood of continuing or discontinuing the beliefs. Reinforcements can exist self-initiated or in the environs, and reinforcements can be positive or negative. This is the construct of SCT that most closely ties to the reciprocal relationship betwixt behavior and environment.
- Expectations - This refers to the anticipated consequences of a person's beliefs. Outcome expectations can exist health-related or not wellness-related. People anticipate the consequences of their actions before engaging in the beliefs, and these predictable consequences tin can influence successful completion of the behavior. Expectations derive largely from previous experience. While expectancies besides derive from previous experience, expectancies focus on the value that is placed on the outcome and are subjective to the private.
- Self-efficacy - This refers to the level of a person'due south confidence in his or her ability to successfully perform a behavior. Self-efficacy is unique to SCT although other theories have added this construct at later dates, such equally the Theory of Planned Behavior. Self-efficacy is influenced by a person'southward specific capabilities and other individual factors, as well every bit by environmental factors (barriers and facilitators).
Limitation of Social Cognitive Theory
At that place are several limitations of SCT, which should be considered when using this theory in public wellness. Limitations of the model include the following:
- The theory assumes that changes in the surroundings will automatically atomic number 82 to changes in the person, when this may not ever be true.
- The theory is loosely organized, based solely on the dynamic interplay between person, beliefs, and environment. It is unclear the extent to which each of these factors into bodily behavior and if one is more influential than another.
- The theory heavily focuses on processes of learning and in doing so disregards biological and hormonal predispositions that may influence behaviors, regardless of past experience and expectations.
- The theory does not focus on emotion or motivation, other than through reference to past experience. In that location is minimal attending on these factors.
- The theory can be broad-reaching, so can be difficult to operationalize in entirety.
Social Cerebral Theory considers many levels of the social ecological model in addressing behavior change of individuals. SCT has been widely used in wellness promotion given the emphasis on the individual and the environment, the latter of which has become a major point of focus in contempo years for health promotion activities. Equally with other theories, applicability of all the constructs of SCT to one public health problem may be difficult especially in developing focused public health programs.
The Transtheoretical Model (Stages of Change)
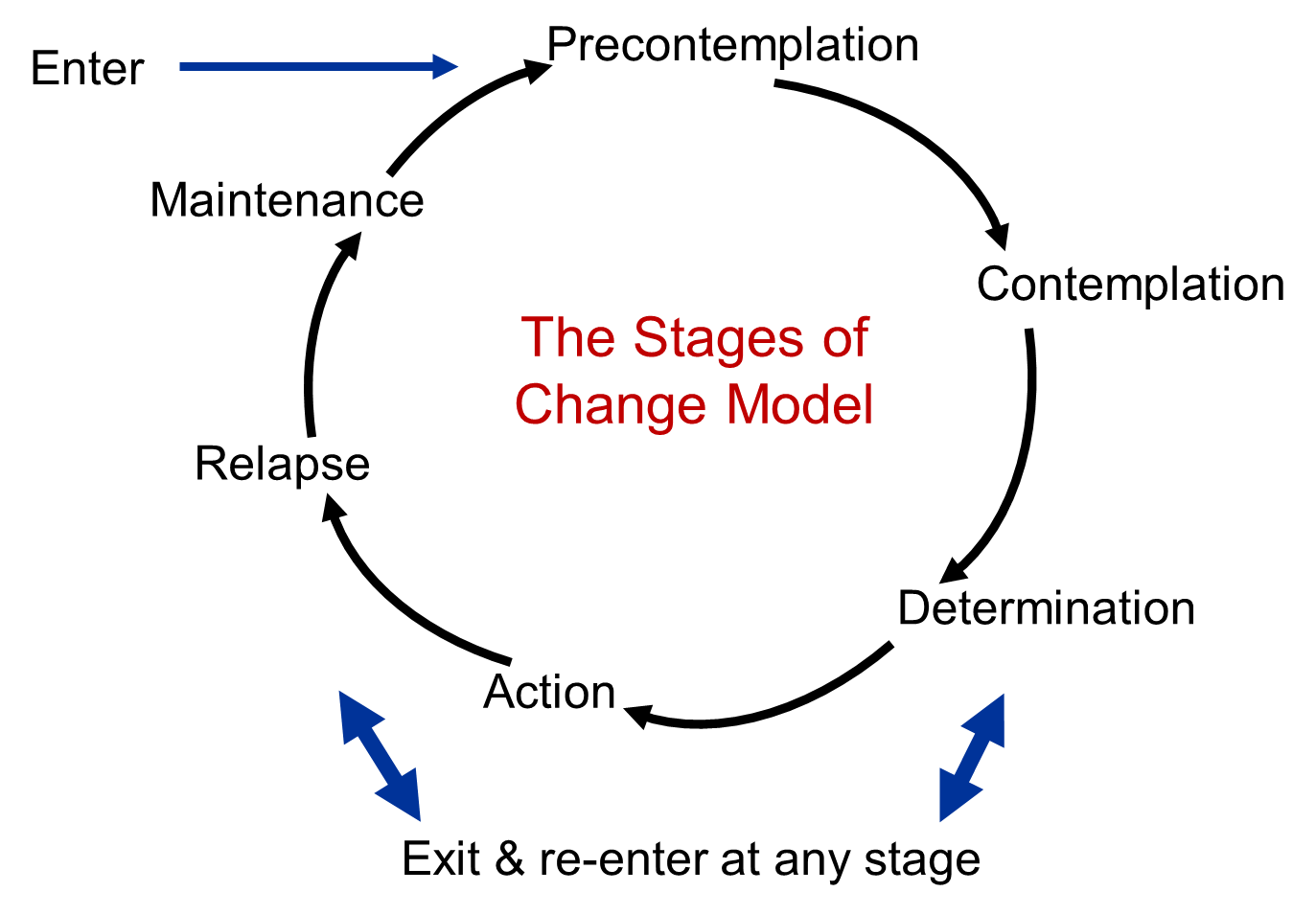
The Transtheoretical Model (likewise called the Stages of Change Model), adult by Prochaska and DiClemente in the belatedly 1970s, evolved through studies examining the experiences of smokers who quit on their own with those requiring further treatment to understand why some people were capable of quitting on their own. It was adamant that people quit smoking if they were ready to exercise so. Thus, the Transtheoretical Model (TTM) focuses on the decision-making of the individual and is a model of intentional change. The TTM operates on the assumption that people do not change behaviors chop-chop and decisively. Rather, change in beliefs, particularly habitual behavior, occurs continuously through a cyclical process. The TTM is not a theory but a model; unlike behavioral theories and constructs tin can be applied to various stages of the model where they may be near effective.
The TTM posits that individuals move through six stages of change: precontemplation, contemplation, preparation, action, maintenance, and termination. Termination was not role of the original model and is less often used in application of stages of modify for health-related behaviors. For each stage of change, different intervention strategies are most effective at moving the person to the next stage of alter and subsequently through the model to maintenance, the ideal stage of beliefs.
- Precontemplation - In this phase, people do not intend to accept action in the foreseeable futurity (defined as within the next half dozen months). People are often unaware that their behavior is problematic or produces negative consequences. People in this stage frequently underestimate the pros of irresolute behavior and place likewise much emphasis on the cons of changing behavior.
- Contemplation - In this stage, people are intending to start the healthy behavior in the foreseeable future (defined as within the adjacent 6 months). People recognize that their beliefs may exist problematic, and a more thoughtful and applied consideration of the pros and cons of changing the beliefs takes identify, with equal accent placed on both. Fifty-fifty with this recognition, people may still feel ambivalent toward changing their behavior.
- Preparation (Conclusion) - In this phase, people are ready to take activeness inside the next xxx days. People start to take pocket-size steps toward the beliefs alter, and they believe changing their behavior can atomic number 82 to a healthier life.
- Action - In this phase, people have recently inverse their behavior (defined as within the last 6 months) and intend to keep moving forward with that behavior change. People may exhibit this by modifying their problem behavior or acquiring new healthy behaviors.
- Maintenance - In this stage, people have sustained their behavior alter for a while (defined as more than 6 months) and intend to maintain the beliefs modify going forward. People in this stage work to prevent relapse to earlier stages.
- Termination - In this stage, people have no want to return to their unhealthy behaviors and are sure they will not relapse. Since this is rarely reached, and people tend to stay in the maintenance phase, this stage is often not considered in health promotion programs.
To progress through the stages of change, people apply cerebral, affective, and evaluative processes. Ten processes of change have been identified with some processes being more than relevant to a specific stage of change than other processes. These processes issue in strategies that help people make and maintain change.
- Consciousness Raising - Increasing awareness about the healthy behavior.
- Dramatic Relief - Emotional arousal virtually the wellness behavior, whether positive or negative arousal.
- Self-Reevaluation - Self reappraisal to realize the healthy behavior is role of who they desire to exist.
- Ecology Reevaluation - Social reappraisal to realize how their unhealthy behavior affects others.
- Social Liberation - Ecology opportunities that exist to show society is supportive of the healthy behavior.
- Self-Liberation - Commitment to change behavior based on the belief that achievement of the healthy beliefs is possible.
- Helping Relationships - Finding supportive relationships that encourage the desired change.
- Counter-Conditioning - Substituting healthy behaviors and thoughts for unhealthy behaviors and thoughts.
- Reinforcement Management - Rewarding the positive behavior and reducing the rewards that come from negative behavior.
- Stimulus Command - Re-engineering the environment to accept reminders and cues that support and encourage the healthy behavior and remove those that encourage the unhealthy beliefs.
Limitations of the Transtheoretical Model
There are several limitations of TTM, which should be considered when using this theory in public health. Limitations of the model include the following:
- The theory ignores the social context in which modify occurs, such as SES and income.
- The lines between the stages tin can exist capricious with no set criteria of how to determine a person's stage of alter. The questionnaires that accept been developed to assign a person to a stage of alter are non always standardized or validated.
- There is no clear sense for how much fourth dimension is needed for each stage, or how long a person can remain in a stage.
- The model assumes that individuals brand coherent and logical plans in their decision-making process when this is not e'er true.
The Transtheoretical Model provides suggested strategies for public health interventions to address people at various stages of the determination-making process. This can result in interventions that are tailored (i.e., a message or program component has been specifically created for a target population's level of knowledge and motivation) and effective. The TTM encourages an cess of an individual's current stage of change and accounts for relapse in people's decision-making process.
Social Norms Theory
The Social Norms Theory was beginning used by Perkins and Berkowitz in 1986 to address educatee alcohol use patterns. As a result, the theory, and after the social norms approach, is best known for its effectiveness in reducing alcohol consumption and booze-related injury in higher students. The arroyo has also been used to accost a wide range of public health topics including tobacco apply, driving under the influence prevention, seat belt use, and more recently sexual attack prevention. The target population for social norms approaches tends to be college students, just has recently been used with younger student populations (i.due east., high school).
This theory aims to understand the environment and interpersonal influences (such every bit peers) in club to alter behavior, which can exist more effective than a focus on the individual to change behavior. Peer influence, and the role information technology plays in private conclusion-making around behaviors, is the primary focus of Social Norms Theory. Peer influences and normative beliefs are especially important when addressing behaviors in youth. Peer influences are afflicted more by perceived norms (what we view as typical or standard in a group) rather than on the actual norm (the existent beliefs and actions of the group). The gap betwixt perceived and bodily is a misperception , and this forms the foundation for the social norms approach.
The Social Norms Theory posits that our behavior is influenced by misperceptions of how our peers think and act. Overestimations of trouble behavior in our peers will crusade us to increase our own problem behaviors; underestimations of problem behavior in our peers will discourage us from engaging in the problematic behavior. Accordingly, the theory states that correcting misperceptions of perceived norms will nearly likely effect in a decrease in the problem behavior or an increment in the desired behavior.
Social norms interventions aim to present correct information about peer grouping norms in an try to correct misperceptions of norms. In particular, many social norms interventions are social norms media campaigns where misperceptions are addressed through customs-wide electronic and impress media that promote authentic and salubrious norms about the wellness beliefs. The phases of a social norms media entrada include:
- Assessment or collection of information to inform the message
- Selection of the normative bulletin that will exist distributed
- Testing the bulletin with the target grouping to ensure it is well-received
- Selection of the way in which the message volition exist delivered
- Amount, or dosage, of the bulletin that volition be delivered
- Evaluation of the effectiveness of the bulletin
Social norms media campaigns are currently beingness funded by many federal agencies, state agencies, foundation grants, and non-profit organizations. Sometimes social norms media campaigns are funded by industry. There has been a proficient deal of evaluations conducted on social norms campaigns. Instance studies of effective social norms campaigns can be found hither: http://world wide web.socialnorm.org/alphabetize.php.
At that place are several limitations of Social Norms Theory that need to be considered prior to using the theory. Limitations of the theory include the following:
- Participants of an intervention focused on social norms are likely to question the initial message being presented to them due to misperceptions they hold. Information must exist presented in a reliable way to correct those misperceptions.
- Poor data collection in the initial stages can lead to unreliable data and poor choice of normative message. This can undermine the entrada and reinforce misperceptions.
- Unreliable sources, or sources that are not credible to the target population, tin event in an unappealing message that undermines the campaign, fifty-fifty if the message is correctly chosen.
- The dose, or amount, of the bulletin received by the target population must be enough to brand an impact, but not too much that it becomes commonplace.
Although these limitations exist, when used correctly Social Norms Theory can be very effective in irresolute individual behavior past focusing on changing misperceptions at the group level. Social norms interventions tin be used alone or in conjunction with other types of intervention strategies. The near effective social norms interventions are those that have messages targeted to the at-risk population that are correct and influential. To target letters, a substantial amount of research and data collection has to be invested to understand the norms that exist in the group of involvement. Social norms interventions are also virtually effective when presented in interactive formats that actively engage the target audition.
Source: https://sphweb.bumc.bu.edu/otlt/mph-modules/sb/behavioralchangetheories/BehavioralChangeTheories_print.html
0 Response to "Which Theory Supports the Idea That Health Behavior (Good or Bad) Can Be Learned by Watching Others?"
Post a Comment